Neck Issues

Neck Issues
The neck has been overlooked for many years as a significant concern for horses, that has all changed. We recognize the importance of this structure for normal activities such as grazing or pulling hay from a net, for balancing in all activities such as getting down or up from the ground and especially for successfully flexing, extending and rotating which are essential motions for all disciplines. If unable to move in all directions these limitations will impact a horse’s movement and soundness. this may develop secondarily to problems located elsewhere or it may be a primary concern. This is where we have our work cut out for us, first identifying it as a factor, then being able to visualize issues with it diagnostically and finally find methods to treat or manage the condition.
The issues that can arise from neck related problems are many and it's not always clear that this is the primary problem. In fact more often than not its inclusion on the list of possible causes of a horse's issue whether an actual lameness or performance related may require ruling in or out many other causes. As we delve into some of the culprits of performance related issues there is an exhaustive list that through evaluating history, presenting signs, diagnostic procedures and therapeutic responses all help us to arrive at a diagnosis. While the diagnostic logarithm requires some work, we at least know now that the neck unquestionably needs to be included in the differentials.
It's interesting to look at the anatomy as that's where it all begins. The vertebrae take an unusual course through the neck as they travel much lower than many expect and so much more of the neck is made up of the musculature plus ligaments. In the following picture you can see what the neck looks like without the skin.
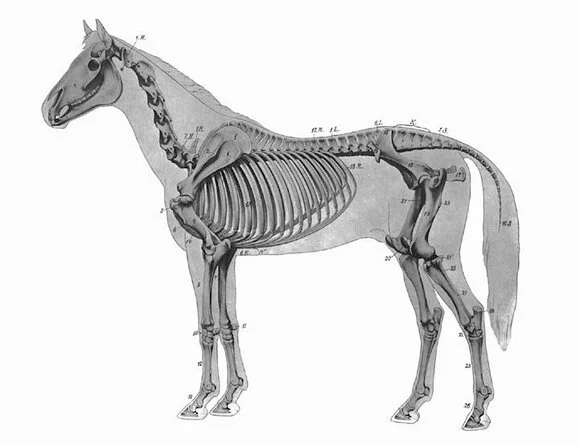
See the “s” curve to the horse’s neck and how low the neck vertebrae go as they meet with the shoulder.


Deep to the muscles are the ligaments that attach the neck vertebrae to the Nuchal ligament.
Examples of Neck Cases
Over the past several years as I have been documenting more patients with neck related issues I wanted to present a few of those here. These are representative of the type of cases that I'm seeing fairly often at this point. While I will try to give at least a summary of the presenting signs it's worth keeping in mind that although aspects of them may fit with your horse, it doesn't mean you have the same disease. Again, there are a myriad of causes for some of these condition's, I'm focusing on ones I know relate to the neck.
I will break these cases up in to three larger categories: Neurologic, Poll Related and Arthritic-Degenerative conditions.
1. Neurologic Cases:
There are times when it's obvious that there are neurologic deficits that a horse is exhibiting. Perhaps they look very weak behind, stumble frequently, have an inability to coordinate their stride and/or mix their gaits where they may be trying to trot in front while doing an irregular canter behind. In any case those horses could have an infectious cause for that condition, a structural one that involves the neck vertebrae and/or a traumatic issue located elsewhere in the body. It's the middle category that I want to focus on. Again anatomy is always important to at least give you an idea what we are trying to describe.

In the above picture the main thing to consider is the alignment and how the floor from one vertebrae moves seamlessly from one to the other and the same is true for the line representing the roof. If the spinal cord can travel unimpeded through these spaces and in turn carry essential neurologic information to and from the brain then all is where it should be. It's when we have disruptions in this alignment that problems develop. As always there are numerous causes: developmental conditions that began with growth, trauma and inflammation to name just a few.
Once again some of the cases I am interested in here are not the more severely affected neurologic horses, but rather the ones that are having performance related issues. An example of one of those is the following: This Arabian mare was sound, willing to be ridden yet having some consistent canter lead issues. Training was considered the most likely issue, but with time and lack of resolution we looked at other causes: saddle fit, back related issues and ulcers. Over time a pattern started to emerge as neck positioning by the horse seemed to correlate with the ability to get the lead or not. I've seen others present similarly where they turn the neck in a particular direction to facilitate getting more normal movement behind.
The next steps were to take survey radiographs of the neck. For those I took views from the poll to the shoulder area in order to see all 7 neck or cervical vertebrae and to assess their alignment. If you compare this radiograph below with the one above you will see there is a "step" (small red arrows) between the bones and that was considered a potential concern.

Another objective method to evaluate the vertebrae and the adequacy of the opening for the passage of the spinal cord is by using a ratio demonstrated in the following radiograph of a different horse. Some of you may have seen me do this calculation in the field as it's an easy screening tool for the likelihood of problems in this area. Anything greater than or equal to 52% is considered normal, thus this horse with a ratio of 45% would certainly be suspect of having a problem.

Now with the information from the above radiographs and the possibility that this could disrupt the flow of neurologic information due to spinal cord impingement, a myelogram would be the next step. This is a procedure where the horse is placed under general anesthesia and a dye is injected into the space of the spinal canal that is outside of the spinal cord. The dye is visible though x-rays so this allows one to tell if there truly has been impingement or not. While viewing the study radiographs are done with the neck in a straight or neutral position then flexed and extended. The following are myelogram pictures from the Arabian horse that was suspicious for spinal cord compression that I referred to New England Equine in Dover, NH several years ago for a study.



Following this evaluation a neurologist questioned whether this was relevant enough to explain the condition. Unfortunately the horse had become less consistent with work and safety concerns developed for the rider. Much of the work for this horse required positioning the neck in a flexed position thus exacerbating the problems already affecting this narrowed space. It was determined that although some horses may function OK with this finding this horse was not one of them and we finally had an answer as to what had been the underlying issue.
Not all horses that are suspect for these issues get a myelogram and unfortunately without that it can be difficult to conclusively know whether impingement is involved or not. If a horse is allowed to work in a manner where they determine their neck position, that is, they are not being asked to flex their necks in or to be on the bit then many of these cases would not be so easily recognized.
2. Poll issues:
Most of you know where the poll area is located, but just to add to that information, the region starts from from the base of the skull and includes the first two vertebrae: CV1 (commonly called the Atlas) and CV2 (commonly called the axis). Between these bones and the ligament which runs above it is a bursa, a fluid filled pouch, that allows for the smooth transit of this ligament (Nuchal Ligament) over these bones as the horse lowers and raises his or her head. Poll problems are often considered especially with dressage horses, but breeds such as Morgans, Arabians and Saddlebreds also need to be considered as so much of their flexion is happening in the poll area.
The following two pictures should help show these structures and they are a good reference when discussing poll issues.


There are 3 horses from the recent years seen by me that are good examples of patients with poll issues and their problems were different yet similar in presentation. They all had flexion issues with the poll area and would avoid keeping a flexed position without some avoidance moves. The first showed a reaction where the Nuchal Ligament attached to the back of the skull, the 2nd showed a rather large fragment that had been pulled away from the back of the skull and had affected the tendons and ligaments that attach there and the 3rd involved a case of bursitis.
In the First Case this mare would allow neck flexion to a point then unexpectedly flip her head, refuse to stay in a frame and be unable to continue with dressage training. By doing x-rays and ultrasound I was able to visualize a reaction along the base of the skull that was consistent with bone inflammation secondary to the pull of the soft tissues on this area. By evaluating with the ultrasound thickness of the soft tissues and an irregular fiber pattern indicated this was the underlying problem. This can best be demonstrated by the following radiograph:

Radiograph demonstrating bone reaction and suspected soft tissue involvement with issues associated with poll resistance.
Once this was found and the combination of a bone reaction along with soft tissue involvement was documented, I proceeded to treat the area by using the ultrasound to visualize the placement of a needle then the area was injected with anti-inflammatories. Fortunately the mare responded well and was able to successfully continue with dressage training.
The Second Case is interesting for several reasons as it was illustrative of how what may seem so obvious may not necessarily be the issue. This horse had a longstanding issue with intermittently head flipping that could go from mild to very pronounced whereby the nose would be thrown in the air and all rider contact would be disrupted. This was especially evident at the canter as he would at times flip his head, thus contorting his upper neck with a fairly dramatic twist and travel inverted. Again not every horse has so dramatic of a problem, but this one did.
Was this from the horse trying to avoid contact, having an issue related to dentistry problems, having an acute pain response somewhere in his body (ie back, neck, poll), experiencing a version of "headshaking" - a syndrome that causes involuntary head shakes or nods, and/or just being difficult? These were all possibilities and undoubtedly quite a few more. There was no question that he was completely sound, he wasn't considered a difficult horse with respect to training issues and his dental exam was unremarkable. So those rule outs at least got me to looking for other physical causes. There was back sensitivity and for those of you that have read the article on Kissing Spine disease this radiograph will demonstrate that this was at least present.

So great we have that here and perhaps that's the answer it could make sense with some of the history. Rather than stop there I decided to look further as this would be a rather extreme reaction for a horse with this milder form of Kissing Spine Disease. Next I x-rayed from the poll to the lower cervical neck vertebrae and found the following in the poll:


Large irregular bone fragment from base of skull.
Now you're probably thinking we have our answer and I would have liked to have thought so as well. The problem is that there is an irregular reaction with respect to the head tossing. Yes, it has been present for over a year, but why wouldn't a fragment this large and one that was definitely affecting the tendons and ligaments as was seen on ultrasound, be a fairly regular problem for this horse? There were occasions I had seen him work where he seemed comfortable, did not object to head positioning and would take the canter and maintain leads without any issue. One of the last rule outs for this horse was the Headshaking condition that I referred to earlier. There are multiple issues associated with this and although I don't want to go into all of them with this article, suffice it to say that it is at times a poorly understood condition that presents itself as an involuntary movement in a horse's head and can be affected by light and temperature. Options for this horse were: start a treatment for Headshaking, treat the poll area +/- inject the Kissing Spine region plus surgery. I consulted with a surgeon at Tufts regarding the fragment and removal was also considered a reasonable option. Naturally, nothing is easy. So I tried a course of medication for headshaking and maybe it helped some, but it wasn't enough to convince any of us that was the whole answer.
So from here I attempted to block or numb the area, but unfortunately due to its location so close to the spinal cord this was problematic. This is one of those cases I can't tie up for you in a neat package and present the final outcome as being as perfect as I would always hope for. It's the nature of the business we work in that there are a number of factors involved and while the headshaking may be part of it I can't rule either it or the fragment out as contributing issues. Mainly it was interesting to see what could be found going through the diagnostic steps.
The Third Case was unusual in its presentation and involved multiple structures in the poll area. The horse was seen in the morning by the groom and he was unable to comfortably flex his head and neck. The night before he went into his stall uneventfully and wore his cribbing strap as he normally did.
When I first saw him that day he was in fact very reluctant to flex his neck laterally or to bring his nose closer to his chest. In addition, he was guarded about any pressure involving the poll area. The following radiograph was taken. By now you probably have a sense of what looks typical of the poll area and this one mainly has one finding which is pointed out with the arrows.

While this was interesting it did not really explain the problem that we were seeing. it was the ultrasound that helped the most with this case. Normally an ultrasound of this area will show no to only a slight amount of fluid in the bursa (appears as black). In this situation the fluid volume is significantly increased.


One of the main concerns for a bursitis in this area is infection so fluid was drained once a needle was placed into the bursa using the ultrasound as a guide and a sample was submitted to a lab.
The good news was that there was no infection, rather a bursitis from an unknown cause. It was interesting in discussing this case with a surgeon from Tufts Veterinary School, Dr. Jose Garcia-Lopez, who has published numerous articles on this condition, that there seems to be a possible correlation between some (not all) horses that wear a cribbing strap and this condition.
The recommendation was surgery which would help to remove the fluid and to reduce the inflammation in the bursa. The surgery was done and some of the mineralized fragments were removed.
In the following 3 pictures you can see what the bursal tissue looks like when the scope is placed into the space. Initially there was an irregular amount of white tissue that was contributing to the fluid build up. In the first 2 pictures an instrument is used to "clean up" this tissue and in the 3rd image a healthier, pink lining is left:



In the end surgery was absolutely the way to go, he remained comfortable without the increased pressure from the fluid in the bursa and got back to being ridden and had full range of motion throughout his neck and poll area. The role that cribbing straps play in this is not clear as there are many horses that wear them without incident. This is one of those cases where it may be related and I'm certainly not suggesting that horse's not wear them, it's just their location over the poll and bursal area is a possible connection.
3. Degenerative Conditions of Neck Vertebral Joints:
This is the area that has probably got the most attention in the past 10 years with more articles written about it in lay journals such as The Horse, professional journals as well as discussed through many veterinary list serves. Essentially it was a long overlooked area as one contributing to problems related to head carriage, front end lameness and disunited gaits behind. Of course these are broad categories and there are many possible contributing factors from training issues to physical ones. In this discussion I will focus on the physical ones related to the neck.
Lack of hind end propulsion could be an issue related to hind end problems, but it could also be related to back comfort as well as the neck. So how do we start when problems arise? There are times when presenting signs can clearly steer me one direction or another and there are others where keeping an open mind as to an ever growing list of differentials needs to be considered.
As a brief overview of anatomy of cervical vertebrae the following picture should help identify the important structures:
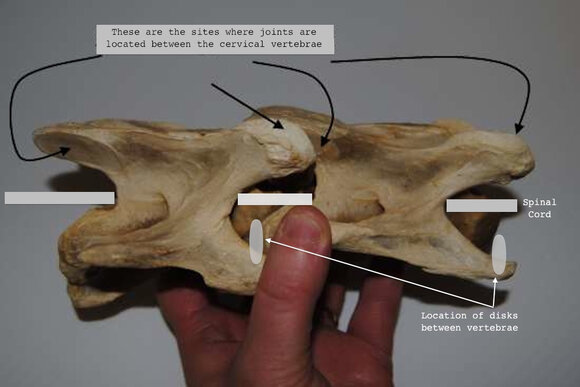
The joints are on the left and right sides of each vertebral pair, below this is the opening for the spinal cord to transit through a protected passage along with sites for the spinal nerves to leave and below that is the disk between each pair.

In this discussion of degenerative changes involving the vertebrae I will be looking at these joints. Now whether we are discussing hocks, fetlocks or coffin joints these are all joints just like those of the neck vertebrae; therefore, they are subject to many of the same problems. Of course the neck doesn't typically get the impact issues related to joints of the lower limb, but they do sustain trauma from overstretching and with falls there can be significant trauma from many forces. What's difficult with the neck is that we don't generally look at it as frequently as other joints so it's more difficult to determine when and what factors precipitated the change. Once the degenerative or arthritic process starts it generally progresses, but at what rate and to what extent is unknown. I have seen some of the changes in horses 8-10 years of age with no known history of problems as well in those much older. Loss of neck flexibility, head carriage issues, reaction to training that involves neck flexion and/or attitude changes associated with bending could be some of the signs. Again, some of these are general categories and other things could be involved as well.
I will post a few cases of horses with different levels of problems and how they were managed.
The radiographs below are from 2 horses with similar problems with respect to limited neck flexibility. The 1st was a mare who trained in dressage work, but kept having issues with her neck flexibility and throughness. I injected her neck joints several times and her response was quite good. Fortunately these changes were not too severe.

The 2nd horse was a gelding that I was evaluating for a soundness exam two years before. He was uneven in front and this seemed to mostly show up in the more anterior phase of his stride especially when not connected. Radiographs demonstrated the arthritic type change around the joint and I injected his vertebrae also with corticosteroids. Fortunately this resolved the lameness and since then it has not been evident.

This next patient was one of the most dramatic ones and had a history of forelimb lameness, stumbling and difficulty keeping his leg extended for the farrier.

Originally I injected his neck vertebral joints in this area, but there was so much degeneration the improvement was limited and short term. The stumbling had continued and because neurologic concerns were more prevalent I consulted with a surgeon to look at other options. We knew there was degeneration and we were aware that this had progressed deeper into the bone and away from the joint margins so we were assuming that we were getting neurologic issues because the problem was affecting the spinal nerves. This case was referred to New England Equine where Dr. Mike Davis worked with a surgeon from California who flew in to perform the surgical stabilization of this joint. The procedure is called a basket surgery and the goal is to allow fusion and ultimately stabilization of the 2 joints and limit further progression. In the following x-ray you can see what this looked like post surgery.

As far as the outcome, it had mixed results. The horse still had neurologic impairment, but we felt there was improvement in his overall comfort level.
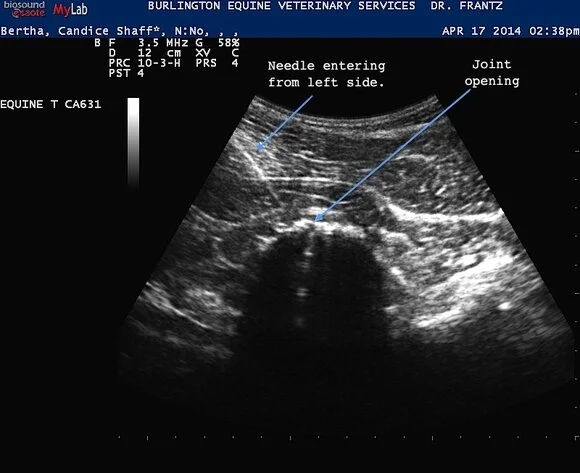
Most of the cases I see are more like what was seen in the previous x-rays and fortunately they are much more amenable to treatment. Just to show you what the treatment looks like here are two ultrasound images of a needle that I am using to inject that’s being guided to the vertebral joint. Ultrasound allows the visualization of the affected structures and at the same time provides real time images as I can see where the needle will be placed.

Like any story sometimes it's hard to know when to stop. I think this gives enough of an overview of some of the types of neck conditions, how they are often presented and the the diagnostic and therapeutic approaches used. The more advanced training with ultrasound plus exploring different treatment regimens have made these easier to understand, visualize and manage.
